Hammer Toes Causes Treatment
 Overview
Overview
A hammer toe can be defined as a Hammer toe condition that causes your toe to bend downward instead of pointing forward. While it can occur on any toe on your foot, it usually affects the second or third toe. If your baby toe curls instead of buckling, it is also considered a hammer toe. There are two types of hammer toes. If your toes still can move around at the joint, then it is considered a flexible hammer toe. It is a milder form of the condition and there are more treatment options. The other type is called a rigid Hammer toes, which occurs when the tendons in your toe become so rigid that they push your toe joint out of alignment, and it cannot move at all. Typically, you will need surgery to fix it.
Causes
Hammer toe results from shoes that don't fit properly or a muscle imbalance, usually in combination with one or more other factors. Muscles work in pairs to straighten and bend the toes. If the toe is bent and held in one position long enough, the muscles tighten and cannot stretch out. Shoes that narrow toward the toe may make your forefoot look smaller. But they also push the smaller toes into a flexed (bent) position. The toes rub against the shoe, leading to the formation of corns and calluses, which further aggravate the condition. A higher heel forces the foot down and squishes the toes against the shoe, increasing the pressure and the bend in the toe. Eventually, the toe muscles become unable to straighten the toe, even when there is no confining shoe.
 Symptoms
Symptoms
Pain on the bottom of your foot, especially under the ball of your foot, is one of the most common symptoms associated with hammertoes. Other common signs and symptoms of hammertoes include pain at the top of your bent toe from footwear pressure. Corns on the top of your bent toe. Redness and swelling in your affected area. Decreased joint range of motion in your affected toe joints.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
Treating hammertoe involves straightening the toe, making tendons in the toes flexible again, and preventing the problem from returning. Some simple treatments include splinting the toe to keep it straight and to stretch the tendons of the foot. Using over-the-counter pads, cushions or straps to decrease discomfort Exercising the toes to relax the foot tendons (a session with a physical therapist may help you get started with foot exercises) Wearing shoes that fit properly and allow toes plenty of room to stretch out.
Surgical Treatment
Treatment of a severe hammertoe that has become rigid includes surgery. What is done during the surgery depends on how misshapen and inflexible the toe is. The surgeon may make a cut over your toe and release the tendon by cutting the tendon away from the bone. The surgeon may remove a small piece of bone from the toe. The surgeon may realign the tendons to reposition your toe or fasten the bones with pins. Sometimes the surgeon may have to join the bones in the toe. In this case, you will no longer be able to bend the toe, but the toe will be flat.
Bunions Cause And Effect
Overview
 A bunion is a bony enlargement of the joint and surrounding soft tissues at the base of the big toe. The enlargement makes the big toe joint stick out further on the side, and forces the big toe to curve in closer to the other toes. For some people, bunions cause little or no pain. In Canada, women are 10 times more likely than men to have bunions. Managing the condition so that it doesn't get worse is a matter of wearing appropriate footwear, cushioning and supporting the area, and taking pain relievers as required. People with more severe bunions may need more specific treatment, such as surgery.
A bunion is a bony enlargement of the joint and surrounding soft tissues at the base of the big toe. The enlargement makes the big toe joint stick out further on the side, and forces the big toe to curve in closer to the other toes. For some people, bunions cause little or no pain. In Canada, women are 10 times more likely than men to have bunions. Managing the condition so that it doesn't get worse is a matter of wearing appropriate footwear, cushioning and supporting the area, and taking pain relievers as required. People with more severe bunions may need more specific treatment, such as surgery.
Causes
Wearing footwear that is too tight or causing the toes to be squeezed together are the most commonly blamed factor for the cause of bunions and hallux valgus and is undoubtedly the main contributing factor. This probably is the reason for the higher prevalence of bunions among women. However, studies of some indigenous populations that never wear footwear, show that they also get bunions but they are very uncommon. As they do get bunions, factors other than footwear must play a role in the cause, even though footwear is the main culprit for providing the pressure that causes the symptoms.
Symptoms
Just because you have a bunion does not mean you will necessarily have pain. There are some people with very severe bunions and no pain and people with mild bunions and a lot of pain. Symptoms for a bunion may include pain on the inside of your foot at the big toe joint, swelling on the inside of your foot at the big toe joint, appearance of a "bump" on the inside edge of your foot. The big toe rolling over to one side. Redness on the inside of your foot at the big toe joint. Numbness or burning in the big toe (hallux). Decreased motion at the big toe joint. Painful bursa (fluid-filled sac) on the inside of your foot at the big toe joint. Pain while wearing shoes - especially shoes too narrow or with high heels. Joint pain during activities. Other conditions which may appear with bunions include Corns in between the big toe and second toe. Callous formation on the side or bottom of the big toe or big toe joint. Callous under the second toe joint. Pain in the second toe joint.
Diagnosis
Your doctor is very likely to be able to diagnose your bunion simply by examining your foot. Even before that, he or she will probably ask about your family and personal medical history and evaluate the types of shoes you wear. You'll be asked about your symptoms, when they started and when they occur. You may also be asked to flex your toe so that your doctor can get an idea of your range of motion. He or she may order x-rays in order to determine the extent of your deformity.
Non Surgical Treatment
Treatment options vary depending on the severity of your bunion and the amount of pain it causes you. Early treatment is best to decrease your risk of developing joint deformities. Conservative treatment Nonsurgical treatments that may relieve the pain and pressure of a bunion include changing shoes. Wear roomy, comfortable shoes that provide plenty of space for your toes. Padding and taping. Your Podiatrist can help you tape and pad your foot in a normal position. This can reduce stress on the bunion and alleviate your pain.(Obviously pending on footwear selection). Medications. Acetaminophen (Tylenol, others) can control the pain of a bunion. Your doctor may suggest nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (Advil, Motrin, others) or naproxen (Aleve), for relieving pain and reducing inflammation. Cortisone injections also can be helpful. But keep in mind that medications do not alleviate the actual cause of the pain. Physical therapy. The heating effect of ultrasound therapy or whirlpool baths can provide relief from the pain and inflammation of a bunion. Orthotics can help control abnormal movement of your foot, reducing your symptoms and preventing your bunion from getting worse. Over-the-counter arch supports can provide relief for some people, though others may require prescription orthotics. 
Surgical Treatment
The decision to have bunion surgery is personal and different everyone. While there are many reasons to have bunion surgery, the most common reasons include. Pain. Difficulty walking. Difficulty fitting shoes. Worsening bunion. Pain at the ball of the foot. Failed conservative measures. See Non-surgical Treatment. Some people have surgery simply because they don?t like the way the bunion looks. While some doctors may correct your bunion if it doesn?t hurt, you should be aware that permanent pain may occur after your surgery.
Prevention
Here are some tips to help you prevent bunions. Wear shoes that fit well. Use custom orthotic devices. Avoid shoes with small toe boxes and high heels. Exercise daily to keep the muscles of your feet and legs strong and healthy. Follow your doctor?s treatment and recovery instructions thoroughly. Unfortunately, if you suffer from bunions due to genetics, there may be nothing you can do to prevent them from occurring. Talk with your doctor about additional prevention steps you can take, especially if you are prone to them.
The Treatment Of Over-Pronation
Overview
The rolling of the foot is a natural process and the degree to which pronation occurs will depend on an individual?s gait. It has been suggested that up to 70 percent of runners may overpronate to some degree, although it is not always bad for the body even though pronation may not be at optimum levels. Slight overpronation may be perfectly acceptable and may not place an individual at an increased risk of injury; however determining whether this is the case can only come from a doctor, podiatrist or sports therapist. While specialist running shoe stores may be able to spot whether you are an overpronator after observing you on a treadmill and suggest the best running shoes to suit your gait, it is still wise if you are an overpronator to get your gait checked professionally.
Causes
A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development.
Symptoms
If ignored, overpronation can lead to complications such as hammer toes, corns and calluses, shin splints, hallux rigidus and many more foot and lower leg problems. Hammer toes appear when the toes are placed under too much pressure and the ligaments and muscles in the toes begin to reduce in size, leading to the curvature of the toes and making them look like little hammers. Overpronators can develop hammertoes if they don?t wear an appropriate pair of shoes. Corns and calluses also appear as a result of overpronation. They form in response to excess pressure, and overpronators may find that they have excessive hard skin on the balls of the feet and inside edge of the big toe. It is the body?s way of protecting against excessive forces and friction. They can be painful.
Diagnosis
Bunions, calluses and crooked toes may indicate alignment problems. So, it is important to ascertain the condition of a client's toes. Check the big toe to determine if the first joint of the toe is swollen, has a callus or bunion, and/or looks as though it abducts (i.e., hallux valgus) rather than pointing straight ahead. Also, look to see if the lesser toes seem to "curl up" (i.e., the person has hammer or claw toes). This may be indicative of damage to, or inflexibility of the plantar fascia caused by excessive flattening of the foot.
Non Surgical Treatment
Mild cases of Overpronation may be controlled or corrected with a supportive shoe that offers medial support to the foot along with a strong heel counter to control excessive motion at the heel starting with heel strike. In mild cases with no abnormal mechanical pressures, an over the counter orthotic with heel cup and longitudinal or medial arch support to keep the foot from progressing past neutral may help to realign the foot. A Custom foot orthotic with heel cup and longitudinal arch support to help correct position of the foot as it moves through motion. Heel wedges may also assist in correcting motion.
Prevention
Strengthen the glutes to slow down the force of the foot moving too far inward. Most individuals who over-pronate have weak glute muscles and strengthening this area is a must. A simple exercise to strengthen glutes is lateral tube walking across a field/court/room. Place a lateral stretch band around your ankles and move your leg sideways while keeping your feet forward.
The rolling of the foot is a natural process and the degree to which pronation occurs will depend on an individual?s gait. It has been suggested that up to 70 percent of runners may overpronate to some degree, although it is not always bad for the body even though pronation may not be at optimum levels. Slight overpronation may be perfectly acceptable and may not place an individual at an increased risk of injury; however determining whether this is the case can only come from a doctor, podiatrist or sports therapist. While specialist running shoe stores may be able to spot whether you are an overpronator after observing you on a treadmill and suggest the best running shoes to suit your gait, it is still wise if you are an overpronator to get your gait checked professionally.
Causes
A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development.
Symptoms
If ignored, overpronation can lead to complications such as hammer toes, corns and calluses, shin splints, hallux rigidus and many more foot and lower leg problems. Hammer toes appear when the toes are placed under too much pressure and the ligaments and muscles in the toes begin to reduce in size, leading to the curvature of the toes and making them look like little hammers. Overpronators can develop hammertoes if they don?t wear an appropriate pair of shoes. Corns and calluses also appear as a result of overpronation. They form in response to excess pressure, and overpronators may find that they have excessive hard skin on the balls of the feet and inside edge of the big toe. It is the body?s way of protecting against excessive forces and friction. They can be painful.
Diagnosis
Bunions, calluses and crooked toes may indicate alignment problems. So, it is important to ascertain the condition of a client's toes. Check the big toe to determine if the first joint of the toe is swollen, has a callus or bunion, and/or looks as though it abducts (i.e., hallux valgus) rather than pointing straight ahead. Also, look to see if the lesser toes seem to "curl up" (i.e., the person has hammer or claw toes). This may be indicative of damage to, or inflexibility of the plantar fascia caused by excessive flattening of the foot.
Non Surgical Treatment
Mild cases of Overpronation may be controlled or corrected with a supportive shoe that offers medial support to the foot along with a strong heel counter to control excessive motion at the heel starting with heel strike. In mild cases with no abnormal mechanical pressures, an over the counter orthotic with heel cup and longitudinal or medial arch support to keep the foot from progressing past neutral may help to realign the foot. A Custom foot orthotic with heel cup and longitudinal arch support to help correct position of the foot as it moves through motion. Heel wedges may also assist in correcting motion.
Prevention
Strengthen the glutes to slow down the force of the foot moving too far inward. Most individuals who over-pronate have weak glute muscles and strengthening this area is a must. A simple exercise to strengthen glutes is lateral tube walking across a field/court/room. Place a lateral stretch band around your ankles and move your leg sideways while keeping your feet forward.
Find Out How To Spot Severs Disease?
Overview
Sever's Disease is a serious type of 'growing pain' rooted in the fact that the rate of growth of a child's heel bones is slower than that of the ligaments of the leg. The heel bone is one of the first bones in the human body to reach full size, and it is prone to injury because it is not flexible or elastic. As a child goes through growth spurts of the heel bone, the Achilles tendon, which connects the calf muscle to the heel, may be struggling to play catch-up, due to its slower rate of growth. In this scenario, the tendon and leg muscles can become strained, tight and over-stretched. As the child walks, runs or plays, repetitive pressure is placed on the tendon, and the tension can cause damage to the growing heel bone, resulting in pain and inflammation.
Causes
Your child is most at risk for this condition when he or she is in the early part of the growth spurt in early puberty. Sever's disease is most common in physically active girls 8 years to 10 years of age and in physically active boys 10 years to 12 years of age. Soccer players and gymnasts often get Sever's disease, but children who do any running or jumping activity may also be at an increased risk. Sever's disease rarely occurs in older teenagers because the back of the heel has typically finished growing by 15 years of age.
Symptoms
The most obvious sign of Sever's disease is pain or tenderness in one or both heels, usually at the back. The pain also might extend to the sides and bottom of the heel, ending near the arch of the foot. A child also may have these related problems, swelling and redness in the heel, difficulty walking, discomfort or stiffness in the feet upon awaking, discomfort when the heel is squeezed on both sides, an unusual walk, such as walking with a limp or on tiptoes to avoid putting pressure on the heel. Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
In Sever's disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she runs or jumps. He or she may have a tendency to tiptoe. Your child's heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your doctor may also find that your child's heel tendons have become tight.
Non Surgical Treatment
The following are different treatment options. Rest and modify activity. Limit running and high-impact activity to rest the heel and lessen the pain. Choose one running or jumping sport to play at a time. Substitute low-impact cross-training activities to maintain cardiovascular fitness. This can include biking, swimming, using a stair-climber or elliptical machine, rowing, or inline skating. Reduce inflammation. Ice for at least 20 minutes after activity or when pain increases. Nonsteroidal anti-inflammatory drugs (NSAIDs) may also help. Stretch the calf. Increase calf flexibility by doing calf stretches for 30 to 45 seconds several times per day. Protect the heel. The shoe may need to be modified to provide the proper heel lift or arch support. Select a shoe with good arch support and heel lift if possible. Try heel lifts or heel cups in sports shoes, especially cleats. Try arch support in cleats if flat feet contribute to the problem.
Exercise
Exercises that help to stretch the calf muscles and hamstrings are effective at treating Sever's disease. An exercise known as foot curling, in which the foot is pointed away from the body, then curled toward the body in order to help stretch the muscles, has also proven to be very effective at treating Sever's disease. The curling exercise should be done in sets of 10 or 20 repetitions, and repeated several times throughout the day.
Sever's Disease is a serious type of 'growing pain' rooted in the fact that the rate of growth of a child's heel bones is slower than that of the ligaments of the leg. The heel bone is one of the first bones in the human body to reach full size, and it is prone to injury because it is not flexible or elastic. As a child goes through growth spurts of the heel bone, the Achilles tendon, which connects the calf muscle to the heel, may be struggling to play catch-up, due to its slower rate of growth. In this scenario, the tendon and leg muscles can become strained, tight and over-stretched. As the child walks, runs or plays, repetitive pressure is placed on the tendon, and the tension can cause damage to the growing heel bone, resulting in pain and inflammation.
Causes
Your child is most at risk for this condition when he or she is in the early part of the growth spurt in early puberty. Sever's disease is most common in physically active girls 8 years to 10 years of age and in physically active boys 10 years to 12 years of age. Soccer players and gymnasts often get Sever's disease, but children who do any running or jumping activity may also be at an increased risk. Sever's disease rarely occurs in older teenagers because the back of the heel has typically finished growing by 15 years of age.
Symptoms
The most obvious sign of Sever's disease is pain or tenderness in one or both heels, usually at the back. The pain also might extend to the sides and bottom of the heel, ending near the arch of the foot. A child also may have these related problems, swelling and redness in the heel, difficulty walking, discomfort or stiffness in the feet upon awaking, discomfort when the heel is squeezed on both sides, an unusual walk, such as walking with a limp or on tiptoes to avoid putting pressure on the heel. Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
In Sever's disease, heel pain can be in one or both heels. It usually starts after a child begins a new sports season or a new sport. Your child may walk with a limp. The pain may increase when he or she runs or jumps. He or she may have a tendency to tiptoe. Your child's heel may hurt if you squeeze both sides toward the very back. This is called the squeeze test. Your doctor may also find that your child's heel tendons have become tight.
Non Surgical Treatment
The following are different treatment options. Rest and modify activity. Limit running and high-impact activity to rest the heel and lessen the pain. Choose one running or jumping sport to play at a time. Substitute low-impact cross-training activities to maintain cardiovascular fitness. This can include biking, swimming, using a stair-climber or elliptical machine, rowing, or inline skating. Reduce inflammation. Ice for at least 20 minutes after activity or when pain increases. Nonsteroidal anti-inflammatory drugs (NSAIDs) may also help. Stretch the calf. Increase calf flexibility by doing calf stretches for 30 to 45 seconds several times per day. Protect the heel. The shoe may need to be modified to provide the proper heel lift or arch support. Select a shoe with good arch support and heel lift if possible. Try heel lifts or heel cups in sports shoes, especially cleats. Try arch support in cleats if flat feet contribute to the problem.
Exercise
Exercises that help to stretch the calf muscles and hamstrings are effective at treating Sever's disease. An exercise known as foot curling, in which the foot is pointed away from the body, then curled toward the body in order to help stretch the muscles, has also proven to be very effective at treating Sever's disease. The curling exercise should be done in sets of 10 or 20 repetitions, and repeated several times throughout the day.
What Will Be The Causes And Signals Of A Ruptured Achilles Tendon?
Overview
 Complete Achilles tendon ruptures occur most commonly at the mid-substance, but also distally at the insertion site or proximally at the myotendinous junction. These can be traumatic and devastating injuries, resulting in significant pain, disability, and healthcare cost. As many as 2.5 million individuals sustain Achilles tendon ruptures each year and the incidence is rising. This trend is due, in part, to an increase in athletic participation across individuals of all ages.
Complete Achilles tendon ruptures occur most commonly at the mid-substance, but also distally at the insertion site or proximally at the myotendinous junction. These can be traumatic and devastating injuries, resulting in significant pain, disability, and healthcare cost. As many as 2.5 million individuals sustain Achilles tendon ruptures each year and the incidence is rising. This trend is due, in part, to an increase in athletic participation across individuals of all ages.
Causes
An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries.
Symptoms
The pain from an Achilles tendon rupture is usually felt in the back of the lower leg, in the area 2 to 6 cm. above the Achilles tendon's attachment to the calcaneus. Individuals with an Achilles tendon rupture often describe a "pop" or similar feeling at the time of the injury. A "hole" or defect in the Achilles tendon can usually be felt under the skin in this area. A limp and inability to rise up on the toes of the affected foot are usually present. If the affected foot does not plantar flex when the calf muscles are squeezed an Achilles tendon rupture is very likely.
Diagnosis
An Achilles' tendon injury can be diagnosed by applying the Thompson Test (or Calf Squeeze Test) this is where the person who has suffered the injury lies on their front with their legs bent. Whoever is performing the test, usually a doctor, will then squeeze the calf muscle. If the tendon has not ruptured then the foot should point briefly away from the leg.
Non Surgical Treatment
Your doctor may advise you to rest your leg and keep the tendon immobile in a plaster cast while it heals. Or you may need to have an operation to treat an Achilles tendon rupture. The treatment you have will depend on your individual circumstances, such as your age, general health and how active you are. It will also depend on whether you have partially or completely torn your tendon. If you have a partial tear, it might get better without any treatment. Ask your doctor for advice on the best treatment for you. If you need pain relief, you can take over-the-counter painkillers such as paracetamol or ibuprofen. Always read the patient information that comes with your medicine and if you have any questions, ask your pharmacist for advice. 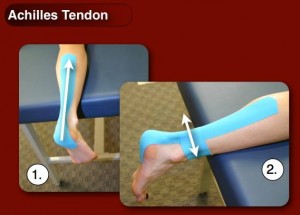
Surgical Treatment
While it is possible to treat an Achilles tendon rupture without surgery, this is not ideal since the maximum strength of the muscle and tendon rarely returns. The reason is the ends of the tendon are ruptured in a very irregular manner, almost like the ends of a paint brush. As soon as the tendon ruptures, the calf muscle (gastrocnemius muscle) continues to pull on the tendon and the end of the ruptured tendon pulls back into the leg, which is called retraction. Once the tendon retracts, it is never possible to get sufficient strength back without surgery, because the muscle no longer functions at the correct biomechanical length and is now stretched out. There are patients for whom surgery cannot be performed, in particular, due to existing medical conditions that may add to potential for complications following surgery. For these patients, a specially designed boot that positions the foot correctly and takes the pressure and tension off the muscle and tendon is used. Most importantly, a cast is never used because it causes permanent shrinkage (atrophy) of the calf muscle. The special boot permits pressure on the foot with walking. The boot also has a hinge to permit movement of the ankle. Many studies of Achilles tendon ruptures have shown that this movement of the foot in the boot while walking is ideal for tendon healing. If surgery is not recommended, it is essential to obtain special tests to check that the ends of the tendon are lying next to each other so that healing can occur. The best test to do this is an ultrasound and not an MRI.
How To Calculate A Leg Length Discrepancy
Overview
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment depends on the amount and cause of the leg length discrepancy as well as the age of your child. Typically, if the difference is less than 2 cm we don?t recommend immediate treatment. We may recommend that your child wear a heel lift in one shoe to make walking and running more comfortable. If the leg length discrepancy is more significant, your doctor may recommend surgery to shorten or lengthen a leg. The procedure used most often to shorten a leg is called epiphysiodesis.

Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment depends on the amount and cause of the leg length discrepancy as well as the age of your child. Typically, if the difference is less than 2 cm we don?t recommend immediate treatment. We may recommend that your child wear a heel lift in one shoe to make walking and running more comfortable. If the leg length discrepancy is more significant, your doctor may recommend surgery to shorten or lengthen a leg. The procedure used most often to shorten a leg is called epiphysiodesis.
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
How To Correct Flat Feet In Adults
Overview
Adult flatfoot (adult acquired flatfoot) or posterior tibial tendon dysfunction (PTTD) is a common pathology presented to foot and ankle specialists. PTTD is characterized by a valgus (everted) hindfoot, flattening of the longitudinal arch of the foot (collapse) and abduction of the forefoot. This is a progressive deformity that begins flexible and can become rigid over time. The posterior tibial tendon (PT) is one of the main supporting structures of the foot arch. Changes within this tendon cause flattening of the foot. There are four stages of this deformity that begins flexible and progressives, with no treatment, to a rigid deformity and with time may involve the ankle joint. Patients usually present with pain in the foot or ankle stating the ?ankle? is rolling. It?s also common for patients to state they have difficulty walking barefoot. Pain is exacerbated after physical activities. Pain is usually isolated to the inside of the foot along the course of the PT tendon. 
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
At first you may notice pain and swelling along the medial (big toe) side of the foot. This is where the posterior tibialis tendon travels from the back of the leg under the medial ankle bone to the foot. As the condition gets worse, tendon failure occurs and the pain gets worse. Some patients experience pain along the lateral (outside) edge of the foot, too. You may find that your feet hurt at the end of the day or after long periods of standing. Some people with this condition have trouble rising up on their toes. They may be unable to participate fully in sports or other recreational activities.
Diagnosis
Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility.
Non surgical Treatment
Nonoperative therapy for posterior tibial tendon dysfunction has been shown to yield 67% good-to-excellent results in 49 patients with stage 2 and 3 deformities. A rigid UCBL orthosis with a medial forefoot post was used in nonobese patients with flexible heel deformities correctible to neutral and less than 10? of forefoot varus. A molded ankle foot orthosis was used in obese patients with fixed deformity and forefoot varus greater than 10?. Average length of orthotic use was 15 months. Four patients ultimately elected to have surgery. The authors concluded that orthotic management is successful in older low-demand patients and that surgical treatment can be reserved for those patients who fail nonoperative treatment. 
Surgical Treatment
Good to excellent results for more than 80% of patients have been reported at five years' follow up for the surgical interventions recommended below. However, the postoperative recovery is a lengthy process, and most surgical procedures require patients to wear a plaster cast for two to three months. Although many patients report that their function is well improved by six months, in our experience a year is required to recover truly and gain full functional improvement after the surgery. Clearly, some patients are not candidates for such major reconstructive surgery.